Radiation injury
Are you looking at radiation injury of :
Radiation injury of the breasts
Frequency
5 years after radiation therapy, 23-27% of patients irradiated with breast cancer are at risk of skin lesion 2. Degree or higher. The risk of chronic pain is 8.4-11.9%. However, 90% of the patients were still satisfied with the results of the radiation therapy .
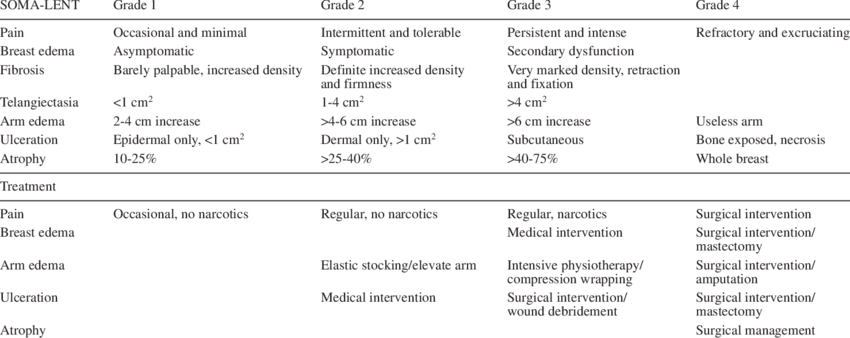
Characteristics of actinic lesions of the breasts.
{kind=link}
Spontaneous evolution
Spontaneous development can be characterized by a slow increase in pain and loss of skin elasticity leading to hardness of the breasts. It can cause painful ulcers that do not heal.
Treatment goal
Improving the aesthetic appearance of the breast, reducing its hardness, eliminating telangiectasia, wound healing, reducing edema of the arm, if any.
Clinical studies
- 2001: 32 patients with radiation damage to the breast received HBOT (only 25 treatments) and 12 did not. HBOT provided significant improvement in skin redness, breast swelling, and breast redness. 7 were completely symptom-free. However, all 12 patients who did not receive HBOT still had the same symptoms.
- 2004: 19 patients who still had arm swelling years after radiation were treated with 30 HBOT. 1 year after treatment, 3 patients had a 20% reduction in arm swelling, 12 patients said their arm had become softer and 6 said they could move their shoulder better.
- 2004: 10 women still with arm swelling up to 9 years after radiation received 20 HBOT. 8 had a 38% reduction in arm swelling 1 year after HBOT. After 20 HBOT, an increase in growth factors was measured.
- 2016: 2538 patients with chronic radiation injury were treated with HBOT. The five most common lesions were osteoradionecrosis (33.4%), dermal soft tissue radionecrosis (27.5%), radiation cystitis (18.6%), radiation proctitis (9.2%), and laryngeal radionecrosis (4.8%). Symptoms improved or disappeared in 76.7% to 92.6% of cases, depending on the type of damage.
- 2016: 57 patients were treated with 47 HBOT for radiation damage to the breast. In addition to better arm mobility, breast swelling, skin ulcers, pain improved in 81% of patients.
- 2018: HBOT does not work against the telangiectasias that appear on the skin after radiation, only the laser can.
- 2019: HBOT leads to a continuous increase of the blood vessels density in the irradiated area.
- 2020: 67 patients were treated with an average of 44 HBOT. 1 year after HBOT, 87% had responded positively to treatment. Pain and skin thickening were better, arm mobility almost doubled afterwards.
- 2021: Patients with radiation damage to the breast underwent surgery. A portion of them received HBOT before and after surgery (total 33 HBOT). Patients who received HBOT before surgery had a lower risk of postoperative complications.
- 2021: Over 1,000 patients with radiation damage to the breast were treated with at least 20 HBOT. The pain, chest and arm discomfort significantly improved 3 months after HBOT. The most common side effect of HBOT was spontaneously resolving myopia in half of cases and mild ear pain in 17% of cases.
- 2022: 13 patients received HBOT 70 months after breast surgery and subsequent breast irradiation. 8 also had chemotherapy. Skin elasticity was measured before and HBOT. HBOT allowed skin elasticity to be almost normalized.
- 2023: This review of the literature found that HBOT is helpful for radiation damage to the breast. However, the studies are rather small and there is a lack of randomized studies.
- 2023: 19 women were treated with 40 HBOT 1 year after surgery in order to improve lymphoedema. Participants reported significant improvements in Quality Of Life (physical functioning, fatigue, insomnia and breast and arm symptoms), with improvements peaking at 6-month follow-up. The results could not been confirmed objective measurements.
Practical use of HBOT
The treatment is used as a mono therapy. As with most radiation injuries, 40 sessions are typically performed.
Radiation injury of the colon (radiation proctitis)
Frequency
Despite modern irradiation technologies, 15% of irradiated patients with the prostate will develop a grade 2 or 3 disease of their rectum (rectitis). Recently an attempt has been made to modulate the intensity of the rays according to the patient, which has allowed only a modest decrease in the rate of radiation rectitis/ proctitis.
Characteristics of radiation proctitis
Bleeding with blood and mucus mixed with stool which can occur months or years after radiation. Diarrhea, stomach pain, bloating, incontinence. The final diagnosis and extent of inflammation is made by colonoscopy and biopsy.
Spontaneous evolution
Heavy bleeding which may require repeated blood transfusions, intestinal incontinence, pain which may require strong analgesics, alternating diarrhea and constipation.
Objectives of the treatment
Stop bleeding, healing of fistulas and infections, normalization of bowel activity, reduction of pain.
Clinical trials
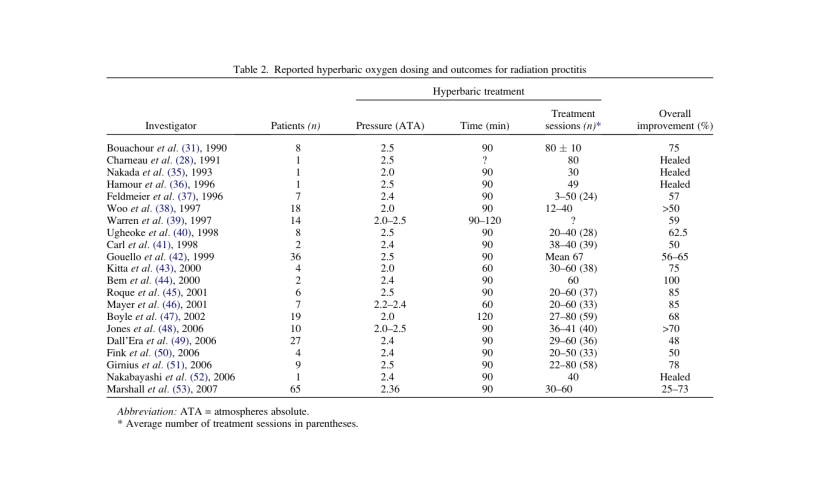
- 2006: 27 men were treated for radiation damage after radiation treatment for prostate cancer. 18 (67%) had healing or improvement of their symptoms with 36 HBOT treatments (29-60).
- More results from 1990 to 2007
- 2007: Significant improvement in radiation proctitis in HBOT patients compared to patients without HBOT.
- 2008: HBOT brings significant improvement in symptoms in 120 patients with radiation proctitis.
- 2008: 13 women with radiation cystitis and radiation proctitis were treated with HBOT. 5 out of 6 women no longer had bleeding and 6 out of 7 women no longer had bladder pain. Scar problems healed in 2 out of 2 women.
- 2012: 11 patients with radiation cystitis had a significant improvement, one of 4 patients with radiation proctitis and severe bleeding could not be helped. The improvement lasted for years.
- 2013: 39 patients with either radiation cystitis or radiation proctitis or both received significant improvement in their symptoms with 36 HBOT (28-40).
- 2013: Radiation injury specialists recommend HBOT for the treatment of radiation cystitis and radiation proctitis
- 2015: 84% improvement in radiation proctitis and 85% in radiation cystitis in a large study from Australia.
- 2023: In this largest cohort reported to date of patients with refractory radiation proctitis treated with HBOT, the overall clinical response rate was 94.3% (including 62.5% complete response) after a median of 60 HBO sessions. Severe intestinal bleeding requires at least 70 sessions.
{kind=link}
Practical use of HBOT
Classical treatments are used for patients with little discomfort. The disease generally heals and further deterioration is avoided. In the event of severe bleeding intestinal radiation, HBOT is administered in addition to hemostatic measures. HBOT can be performed on an outpatient basis. At least 40 sessions take place. Depending on the clinical presentation and the course, additional treatments may be necessary.
Radiation injury of the bladder (radiation cystitis)
Frequency
8 t0 21 % of the patients who have been irradiated for a prostate cancer will develop a radiation cystitis . Radiation cystitis is often associated to a radiation proctitis.
Characteristics of radiation cystitis
Presence of blood in the urine, pain when urinating, frequent and urgent need to urinate, incontinence, social isolation. These signs can occur months or even years after the prostate has been irradiated. The final diagnosis and extent of inflammation is made by cystoscopy and bladder biopsy.
Spontaneous evolution
Increasingly frequent and heavy bleeding which may require blood transfusions, narrowing of the bladder, repeated infections, placement of an artificial bladder.
Objectives of the treatment
Stop hemorrhage, prevent fistulas and infections, improve urinary and bladder function, reduce pain.
Clinical trials
- 1994: Macroscopic hematuria disappeared in 16 of 20 women and improved in 2 with an average of 44 HBOT. Comparison of the cystoscopic findings before and after HBO showed a significant decrease in hemorrhagic sites and telangiectasis of the bladder mucosa.
- 1995: 40 patients with biopsy proven radiation cystitis with 20 HBOT at 3.0 ATA. Bleedings disappeared or improved in 37 patients. Recurrence rate was 0.12 after 2 years of follow-up.
- 2003: 57 patients received an average of 33 HBOT (9-68). 49 had complete or partial resolution of hematuria.
- 2005: 60 patients received an average of 32 HBOT. 80% had partial or resolution of the bleeding, this increased to 96% if the patients were treated within 6 months after the start of bleeding.
- 2012: 38 patients with radiation cystitis were treated with an average of 62 HBOT ± 12. The follow-up period was 11.6 ± 3.7 years. High efficacy ratios of objective and subjective findings were obtained at 2 and 4 (79-95%) years, respectively. After 7 years’ follow-up, these ratios decreased slightly (72-83%) but remained stable thereafter (75-88%) without any serious accident. Early application of HBO treatment after the onset of hematuria appears to produce favorable outcome.
- 2012: The medical costs of a patient suffering from radiation cystitis were followed for 3 years, 6 months before HBOT and 2,5 years after. HBOT reduced costs of inpatient admissions, consultations, investigations, and procedures and provided a projected healthcare saving of 187,483.96 Australian dollars over a 2.5 year follow up.
- 2013: 39 patients were treated with 36 HBOT (28-40). 76% for patients with radiation cystitis, 89% for patients with radiation proctitis, and 88% of patients with combined cystitis and proctitis reported a clear improvement of their EPIC score.
- 2017: 33 HBOT in 38 patients healed the symptoms of radiation cystitis 86,8% of the cases and improved the symptoms in 13.2% of the cases.
- 2019: In this randomized controlled study on an intention to treat base EPIC score was used for assessment. Improvements in the EPIC score were 17.8 in the HBOT (30-40 sessions) group and 7.7 in the control group.
- 2020: A total of 20 papers were obtained, resulting in a cohort of 815 patients who were treated with hyperbaric oxygen therapy for radiation cystitis. The weighted average overall and complete response rates were 87.3% and 65.3%, respectively. Adverse events were observed in 9.6% of the patients, but permanent side-effects were rare.
- 2022: 3 patients who developed grade 3 genitourinary toxicity after a stereotactic radiotherapy were cured with HBOT.
- 2022: HBOT appears to be a safe and effective treatment for refractory hemorrhagic cystitis following chemotherapy and hematopoietic stem cell transplantation.
- 2022: After reviewing 48 publications dealing with the treatment of bleeding caused by radiation cystitis and urethritis the authors recommend HBOT as a first line treatment.
- 2022: The plasma levels of VEGF-A were significantly elevated in radiation cystitis patients and there was a strong trend for significant overexpression in urine. One single HBOT showed a decrease of VEGF-A in patients with radiation cystitis.
- 2022: Unfortunately, radiation-induced hemorrhagic cystitis can lead to persistent or intermittent hematuria. In these cases, intravesical instillation of astringent agents or hyperbaric oxygen therapy can alleviate symptoms.
- 2022: We treated 52 patients, with a median of 30 sessions, for 6 months and 40 months (6-68 months) of follow-up. Reduction of hospitalizations/per year due to hematuria from 2.8 to 1.1 (p=0,001). The 73,5% of patients stated that they were « very much better » or « much better » after treatment.
- 2023: These small studies suggest that for people with late radiation injury affecting tissues of the head, neck, bladder and rectum, HBOT may be associated with improved outcomes (low- to moderate-certainty evidence).
- 2024: Patients with radiation cystitis reported that 39 HBOT improved their hematuria, urinary function and quality of life.
Practical use of HBOT
HBOT is administered as monotherapy in milder cases. In severe hemorrhagic cystitis, HBOT is administered in addition to hemostatic measures. HBOT can be performed on an outpatient basis. There are on average 40 sessions. Up to 60 sessions are performed in more complicated cases.
Radiation injury of the vocal cords
Frequency
Fortunately, this is a rare complication of cancer of the neck or larynx. There are no precise data as to their frequency. Lesions generally begin between 2 months and 25 years after the rays.
Characteristics of lesions of the vocal cords.
Months or years after cancer of the vocal cords, the patient complains of hoarseness, difficulty in swallowing, pain on swallowing, false driving when swallowing food or liquid. The diagnosis is made by the ENT specialist. Without treatment, a laryngeal ulcer can occur, which requires the removal of the vocal cords (laryngectomy). With this operation, one should also expect possible surgical complications, such as fistula formation, wound healing disorders and tracheostomy.
Objective of the treatment
Avoid laryngectomy, maintain the best possible speech quality, close soft tissue fistulas. Classically, actinic lesions are classified according to Chandler. Stage I-II can be treated conservatively Stage III-IV should undergo laryngektomy.
Clinical studies
There are no controlled studies on the treatment of radionecrosis of the vocal cords, regardless of the method of treatment. With a total of 6 smaller publications, mostly in severe cases, hyperbaric oxygen therapy ranks well. Here are the most important studies:
- 1998: HBOT was successful in 5 patients with severe actinic lesions of the larynx. An incurable tracheotomy could be closed with HBOT.
- 2000: the larynx could be saved in 13 of the 18 patients with severe actinic lesions; they were able to keep their voice and could swallow normally.
- 2005: the larynx could be saved in 6 out of 8 patients who worsened despite traditional therapy.
- 2009: in 6 other patients with serious damage to the vocal cords (stage 4 according to Chandler), the larynx could be saved in 5 cases.
- 2013: Hyperbaric oxygen therapy is useful but cannot yet be considered the gold standard.
Radiation injury of the salivary glands
Frequency
Occurs more or less in almost all irradiated patients for cancer of the mouth and neck.
Features
Reduced salivation, which means the patient has to wet their mouth several times with water or a saliva substitute. But it can also be so strong that he can only eat liquid meals .
Diagnosis
It is usually enough for the patient to talk about a lack of saliva after oral cancer to know that he has been irradiated. The diagnosis is definitively made by the ENT or the radiotherapist.
Spontaneous evolution
The decrease or loss of saliva is permanent; it usually begins after a week of radiation.
Purpose of treatment
Saliva substitute and pilocarpine attempt to replace or stimulate saliva with modest results. Recently, attempts have been made to surgically move the salivary glands out of the radiation field before the rays . Hyperbaric oxygen therapy can promote recovery of damaged salivary glands. HBOT allows to improve the microcirculation of the salivary glands and decreases stiffness (fibrosis) of the tongue and neck in rats. Here it is again ‘an action at the genetic level .
Clinical studies
- 2008: 66 irradiated patients treated with HBOT for osteoradionecrosis of the mandible HBOT improved the state of their teeth, had less dry mouth, could better chew and improved their social contacts.
- 2008: 21 irradiated patients were treated with HBOT for osteoradionecrosis of the mandible. Swallowing-related problems significantly decreased and there was a reported subjective increase in saliva quantity and an improvement in sense of taste.
- 2009: Compared to irradiated patients not receiving HBOT, all patients who received it, reported significant improvement in swallowing, dry mouth, sticky saliva, eating in public and pain in mouth.
- 2011: 25 patients of 45 with hyposalivation had a significant increase in whole saliva and 12 regained a normal saliva after HBOT. There was a significant decrease in 69 patients with xerostomia.
- 2011: HBOT increased salivary secretion rate and salivary pH in16 irradiated patients. HBOT also decreased S. mutans and Lactobacillus colony density which may reduce caries progression in those patients.
- 2015: HBOT improved xerostomia in 64% of all patients suffering from osteoradionecrosis of the mandible, soft tissue necrosis of head and neck
- 2018: HBOT improved saliva volume, diminution of discomfort and improved quality of life in 34 patients 12 months after start of HBOT.
Practical use of the OHB
Treatment is used as additional therapy to replace saliva or pilocarpine and general dental care. There are 30 to 40 daily sessions.
Radiation injury to the jaws
Frequency
Rare, should be 1 to 2% (1) with modern radiation technology. Occurs more often in patients who continue to smoke after radiation (2).
Characteristics of radiation damage to the jaws
Non-healing mouth ulcer, pain, throat fistula, tooth loss, facial nerve damage after radiation therapy for oral cancer
Diagnosis
Examination by the maxillofacial surgeon, radiography, MRI, bone biopsy
Spontaneous evolution
Infected, non-healing wounds in the mouth and throat despite antibiotics and surgery. The bone can be so damaged that it can break just by eating.
Objectives of the treatment
Improved wound healing with the result that the operation of the jaw brings a better result, pain relief, prevention of bone fractures
Clinical trials
There are many studies out there, almost all case reports with different experiences: pro (3) , contra (4) . Only a controlled study, but with minor cases, found no argument for a positive effect of HBOT ( 5) . The situation therefore remains controversial (6).
2023: HBOT normalizes gums damaged by radiotherapy to the level of normal healthy gums.
Practical use of OHB
Treatment is used in addition to antibiotics, pain relievers and general care and is considered a tissue improvement measure before any jaw surgery. HBOT can be performed on an outpatient basis. 30 to 60 sessions are usually necessary.
Radiation injury of the brain
Frequency
Very rare, there are few numbers. We are talking about 4.7% of irradiated children over an average period of about 5 years and 9% of adults over a period of one year.
Features
Very variable because it depends on the location of the lesion in the brain. These range from fatigue to headaches, dizziness as well as various complaints such as paralysis, vision problems, balance problems, etc.
Spontaneous evolution
Symptoms remain stable or worsen slowly
Objective of the treatment
Improved blood circulation resulting in improved symptoms over the years. In many cases, the MRI also improves.
Clinical trials
There are no controlled studies. Success has been reported with cortisone, surgery and of course with HBOT.
- 1997: Ten patients suffering from radiation-induced brain injuries, of which eight were confirmed through biopsy, improved after a series of 20-HBOT.
- 2003: HBOT improved symptoms of radiation injury of the brain in a 68-year-old patient after he worsened following 2 months of steroids.
- 2009: HBOT was very successful in 3 cases of radiation injury resistant to corticosteroids after stereotaxic radiosurgery for benign brain tumor.
- 2009: A case report showing the efficacy of HBOT in radiation injury resistant to steroids.
- 2010: HBOT improved both, brain and optic nerve function in 16 women with radiation-induced injuries to their visual pathways, as evidenced by MRI scans. This positive outcome was concomitant with a notable improvement in their vision.
- 2011: HBOT allowed a substantial improvement of neurophysiologic performance in 10 long term of survivors of brain tumor who had received radiation treatment.
- 2014; HBOT improved clinically and radiologically patients with proven radiation injury of the brain, patients also reported subjective improvement.
- 2019: 13 patients with radiation injury to the brain were greatly improved with a combination of steroids and HBOT
- 2020: HBOT improved 12 of 13 patients with radiation injury of the brain. 4 of 8 brain MRI were improved while 4 remained stable.
Practical use of HBOT
As for other actinic lesions, at least 40 daily treatments are applied, lasting 8 weeks.